
 We have collected healthy individual data from over 8’000 persons over the last few years. The data were collected in the Olten area in Switzerland and in the Koblenz area in Germany. From this huge amount of information we are now able to contribute scientific papers about the need for gathering additional information about an individuals risk. View an example of our publication strategy.
We have collected healthy individual data from over 8’000 persons over the last few years. The data were collected in the Olten area in Switzerland and in the Koblenz area in Germany. From this huge amount of information we are now able to contribute scientific papers about the need for gathering additional information about an individuals risk. View an example of our publication strategy.
Our measurement of plaque area is manufacturer independent, encompasses the whole carotid artery from clavicles to lower jaws and not just 6 cm as described elsewhere nor does it need any costly software and the tracings are performed in a few minutes (Figure).
Clinical example
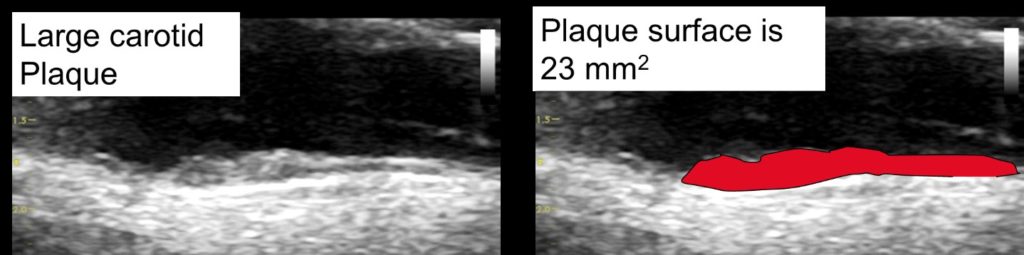
The figure shows the measurement of a plaque area by tracing the longitudinal surface of a carotid plaque (23 mm2). A plaque area of 23 mm2 corresponds to an arterial age of 34 years in men and 43 years in women. Arterial age of 70 years (AA70) corresponds to a total plaque area of 108 mm2 in men and 66 mm2 in women. This represents high risk atherosclerosis: AA70 = 96th percentile for men (sensitivity 9%, specificity 97%) and 95th percentile for women (sensitivity 18%, specificity 95%) in the Tromso study (N=6‘226, follow up 6 years, 297 myocardial infarctions during follow up (2). Bayes posttest risk (13) of VA70 for 4% AGLA: 11% in men, 13% in women, for 10% AGLA: 25% in men and 29% in women. Therefore, AA70 transforms low into intermediate and intermediate into high cardiovascular risk.
Therefore, TPA has great potential for wide-spread use in primary care, since cost of ultrasound machines with included software is below 5’000 € and measurements are very easy to perform. Others use 3D imaging of atherosclerotic plaque, but the clinical use is severly limited by costs, calcified plaque, vendor dependence (Philips iU22 ultrasound system), limited field of view (imaging length of 6 cm with the potential to miss significant amounts of plaque) and need for specialized centers to perform the total plaque volume quantification (reference). Further, the correlation coefficients for 2D-TPA and 3D plaque imaging are good, while the correlation coefficients for IMT and 3D plaque imaging in carotid arteries are very poor (reference).
We previously derived our arterial age risk tool from TPA in 1500 men and women by with substitution of chronological age by vascular age in the PROCAM function and validated this approach externally in a Canadian cohort of 684 primary care subjects with an observation time of 2.6 years in average and where 13 myocardial infarctions occurred (reference): AUC was significantly improved by 0.13 from 0.65 to 0.78 (p=0.02). Therefore, we were able to furnish a validation of our vascular age tool. However, screening subjects aged 40-65 for the presence of old arteries as a gold standard clearly needs further validation.
On this arteris website you get all contemporary information about the urgently needed improvement in cardiovascular risk prediction and atherosclerosis management.